Mandibular surgery : Dalpont- Obwegeser
What is a mandibular osteotomy?
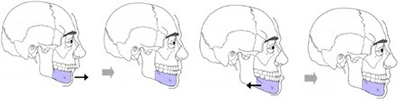
The Dalpont-Obwegeser mandibular osteotomy is the procedure that allows the mobilisation of a part of the lower jaw (the entire lower dental arch and the chin) in order to correct an anomaly in its positioning.
This procedure will therefore correct anomalies of the facial skeleton related to the lower jaw.
This operation is frequently combined with a Lefort I maxillary osteotomy. This is called a maxillo-mandibular osteotomy.
It is often preceded by orthodontic treatment.
The expected benefits of the Dalpont-Obwegeser mandibular osteotomy are
– Restoration of normal tooth relationships and normal masticatory function, thus preventing the risk of long-term dental problems (e.g. loosening of the teeth) or jaw articulation.
– Restoring normal relationships between the two jaws when there is such a mismatch that it is impossible or difficult to propose a dental prosthetic rehabilitation.
– The improvement of the harmony and the global aesthetics of the face from the front as well as from the side.
This operation can therefore correct anomalies such as
- a lower lip and chin that are too far forward,
- a lower lip and chin too far back.
The surgery is performed under general anaesthesia and a hospital stay of about three to five days is necessary.
Pre-operative examinations are essential: blood test, electrocardiogram and in some cases a chest X-ray before the pre-operative consultation with the anaesthetist.
The incision is made in the mouth. It concerns the gum outside the lower molars on both sides. It is therefore invisible; there is no incision in the skin.
Then the two osteotomies (one on each side) are performed, which completely separate the lower dental arch from the rest of the jaw.
The part that has just been separated can then be mobilised in order to reposition it in its ideal position.
This ideal position is determined by various elements
the pre-operative radiological assessment (teleradiography of the skull in profile),
the relationship between the two dental arches, which must be as harmonious as possible (this is one of the main objectives of the operation, the other being to improve the aesthetics of the face). For this reason, a dynamic maxillo-mandibular blocking is very often used. This blocking is done with elastics.
If you have had orthodontic treatment (multi-ring appliance) before the operation, hooks will be placed on the rings to achieve this blocking.
If no orthodontic treatment was necessary, the first stage of the operation will consist of placing a system of arches fixed to the upper and lower dental arches which will allow this blocking to be achieved.
This blocking is kept in place postoperatively for a variable period of time, depending on the case, ranging from a few days to several weeks.
The rest of the operation consists of reattaching the lower dental arch to the rest of the jaw in its new position. This is called osteosynthesis and is carried out using mini-plates and titanium screws.
The procedure ends with the closure of the oral incisions with absorbable thread.
The duration of the operation varies according to the technical difficulties. On average it takes 90 minutes when the mandibular osteotomy is not combined with a maxillary osteotomy.
Post-operative care includes:
– Mouthwash.
– Pain medication (analgesics).
– Medication for swelling (anti-inflammatories).
– Antibiotics are given during the operation and are extended in some cases.
– Application of ice to the cheeks during the first 24 hours (ice has a good anti-inflammatory and anti-edematous effect).
– Food should be liquid for the first few days after the operation, then mixed or ground for the next 5 to 6 weeks.
– Brushing the teeth, even if it is made difficult by the maxillo-mandibular guidance elastics, must remain as careful and rigorous as possible during the post-operative period.
– It is necessary to stop smoking during the post-operative period. Continued smoking favours complications related to poor gum healing.
The post-operative period includes :
– Small amounts of bleeding that may occur in the operated areas during the first 24 hours.
– The pain in the operated areas subsides with the prescribed analgesics and anti-inflammatories and generally disappears in a few days.
– Oedema is frequent and often marked. It is unpredictable and varies from one person to another. In the case of a mandibular osteotomy, it predominates in the lower face and lower lips.
– After unblocking, a painful limitation of the mouth opening is frequent and gradually fades away.
– In the rare cases where the jaws are blocked with steel wires (and not with rubber bands), cutting pliers are prescribed. These should always be kept with you so that you can cut the wires that connect the two jaws in case of an emergency (vomiting).
Sometimes further orthodontic treatment is necessary to correct small imperfections in the dental joint.
Your maxillofacial surgeon may suggest surgery of the nose and/or chin in certain cases and at a distance from the operation when the osteotomy alone does not bring sufficient aesthetic improvement.
Finally, the presence of plates and screws can sometimes become annoying with time. Their removal then becomes necessary during a second operation which will never be performed before the seventh month after the first operation.