Palatal distraction
WHat is palatal distraction?
Palatal distraction is the procedure that gently weakens the entire bony structure that comprises the upper dental arch and widens it to correct a positional anomaly in the direction of the width of the palate.
This procedure will correct anomalies of the facial skeleton related to the upper jaw.
It is always linked to orthodontic treatment after the operation or in some rare cases before the operation.
The expected benefits of palatal distraction associated or not with Lefort I maxillary osteotomy are severalfold
- the restoration of normal relationships between the teeth and of a normal masticatory function, thus preventing the risks of long-term dental problems (loosening or wear of the teeth for example) or of jaw articulation.
- Restoring normal relationships between the two jaws when there is a shift in the transverse direction such that it is impossible or difficult to propose a dental prosthesis.
- the improvement of the harmony and the global aesthetics of the face from the front as well as from the side.
The surgery is performed under general anaesthesia and a hospital stay of about three days is necessary.
Pre-operative examinations are essential: blood test, electrocardiogram and in some cases a chest X-ray before the pre-operative consultation with the anaesthetist.
The incision is made in the mouth. It involves the gum well above the upper teeth. It is therefore invisible from the outside; there is no incision in the skin. The actual osteotomy is then performed, which gently separates the bone structure comprising the upper dental arch into two parts.
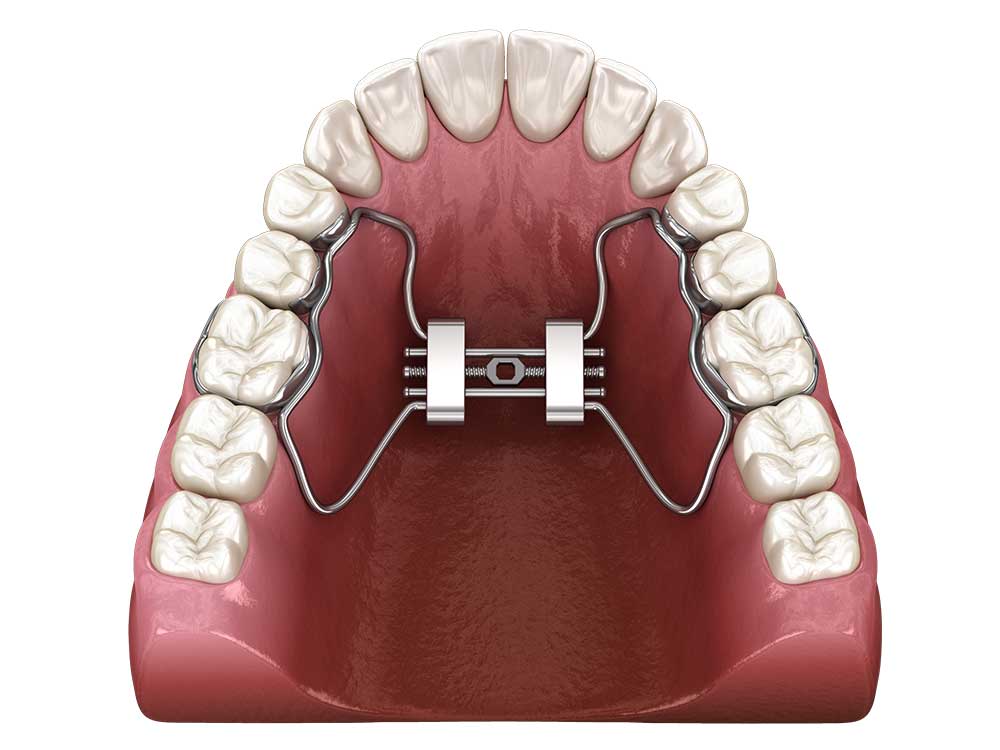
A palatal distractor is fixed with a screw on each side of the palate in the area of the premolars and molars.
The palatal distractor is activated with a key and the widening of the palate results in a central incisor spacing of about 1mm when the patient wakes up.
The duration of the operation varies according to the technical difficulties. On average it takes 60 minutes.
In some cases the wisdom teeth can be removed during the surgery.
The distractor module has three different colours to quantify activation.
Activation usually begins 5-6 days after surgery. The distractor is activated by placing the key in the middle of the module and moving it from the upper incisors to the tongue.
The movement must be repeated until the next colour appears and corresponds to approximately 1/3 of a mm per day.
The patient is reviewed weekly until sufficient activation has occurred, at which time the practitioner places a locking screw to secure the module and prevent deactivation.
The space between the central incisors will depend on the amount of activation and can be several mm or even more than one cm.
The patient should check the stability of the distractor every day, checking that the end colour of the activation is maintained.
Following the operation, the patient presents with facial oedema (swelling) and in some cases haematomas.
Post-operative care includes :
– Mouthwash.
– Pain medication (analgesics).
– Medication for swelling (anti-inflammatories).
– Antibiotics are given during the operation and are extended in some cases.
– Ice is applied to the cheeks for the first 24 hours (ice has a good anti-inflammatory and anti-edema effect).
– Food should be liquid for the first few days after the operation, then mixed or ground for the next 5 to 6 weeks.
– Tooth brushing and maintenance of the distractor with an interdental brush should be as careful and rigorous as possible during the post-operative period.
– The distractor is usually removed under local anaesthetic about three months after the end of activation.
– It is necessary to stop smoking during the post-operative period. Continued smoking can lead to complications due to poor gum healing.
The post-operative period includes :
– Small amounts of bleeding that may occur in the operated areas during the first 24 hours.
– The pain in the operated areas subsides with the prescribed analgesics and anti-inflammatories and generally disappears in a few days.
– Oedema is frequent and often marked. It is unpredictable and varies from one person to another. It predominates in the case of a maxillary osteotomy, in the midface and upper lips.
– A painful limitation of the mouth opening is frequent and gradually fades.
Orthodontic treatment is continued or started approximately 2 months after surgery.